More than 100,000 former foster youth are covered each year by Medicaid as a result of legislative changes that began with the Affordable Care Act, according to a report released this week by the Government Accountability Office.
The report offers no sense of denominator, as in how many could be covered in a given year. But it notes, based on more in-depth interviews with federal and state Medicaid officials, that former foster youth can experience a blend of common and unique barriers to enrollment as they move out of the foster care system.
“Individuals who have aged out of foster care can face barriers to enrolling in Medicaid and maintaining coverage,” the report said. “For example, they may miss Medicaid outreach if they change addresses frequently due to unstable housing, or avoid seeking assistance due to mistrust of state agencies.”
Sen. Ron Wyden, the lead Democrat on the Senate Finance Committee, sought the GAO study. He did not comment specifically on the details of the report. But he said the barriers described in it will only worsen if Republicans seek to cut Medicaid funding, a prospect raised in recent plans for the looming tax reform bill.
“It’s already a challenge for former foster youth to get and keep affordable health insurance,” Wyden said, in an email to Youth Services Insider. “If Republicans have their way and create more barriers to affordable health care, Americans everywhere will suffer, but former foster youth working to build their lives and be independent will be hit especially hard.”
Among the many health care reforms in the Affordable Care Act was a provision putting Medicaid eligibility for youth aging out of foster care essentially on par with a person’s ability to stay on their parent’s private insurance through age 26. Additional legislation several years later tied up a significant loophole where a former foster youth that moved states after exiting care would not be categorically eligible in their new home.
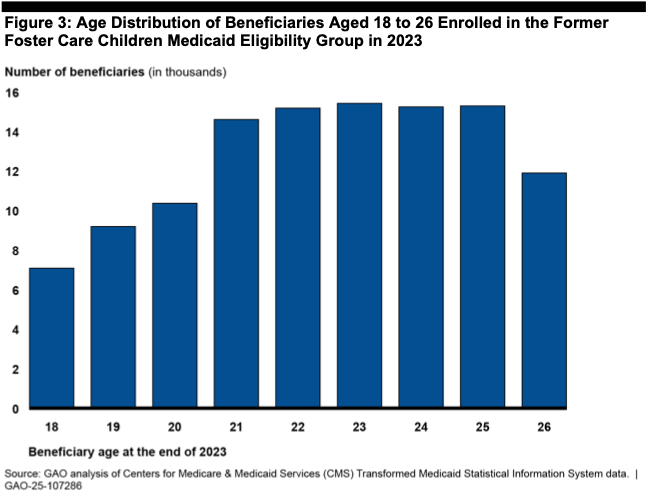
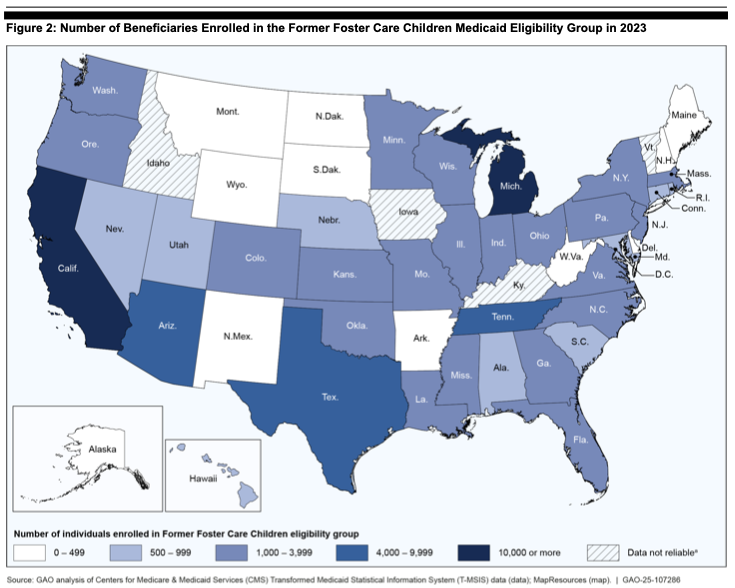
The report analyzes Medicaid data in 46 states (four had systems deemed unreliable) and interviewed federal Medicaid officials, as well as child welfare and health officials in eight states. The analysis found that in 2023, 112,000 former foster youth between the ages of 18 and 26 were enrolled in Medicaid under the eligibility code for former foster youth. This ranged from 70 in Washington, D.C.’s Medicaid program to 26,000 in California. Because the majority of states offer extended foster care through the age of 21, most enrollees were between 21 and 25.
As mentioned before, it is not entirely possible to know how much of the potential universe of former foster youth is accounted for in this 112,000. For starters, some significant portion might have been re-enrolled in a different group, such a pregnant or parenting person, and would not show up in this data.
But back of the envelope, federal data suggests that just below 20,000 foster youth age out into adulthood every year, which would roughly translate to 160,000 people in that 18-26 range at one time. Assuming a good chunk of the 18-21 crowd is remaining in foster care (and thus not yet eligible for post-foster care Medicaid), and factoring in that four states’ Medicaid data was so murky they didn’t count it, it seems this could mean a very high amount of eligible people are getting enrolled.
Report authors say that interviews in the eight states suggest that former foster youth face a lot of barriers that are common to accessing Medicaid, but are more likely to run up against those barriers than the average seeker. These include “difficulties experienced during the Medicaid enrollment and renewal process,” and “frequent address changes due to transient and unstable housing.”
But the report surfaces a few unique issues for foster youth exiting the system, starting with the fact that those who did not have a good experience often mistrust child welfare workers who might be helpful in enrolling them. Also noted as challenges: the lack of specialized knowledge about Medicaid enrollment that is bred by high turnover of workers both in health and child welfare, and difficulty in coordinating between state agencies.